Studies on the link between violence within the couple (VSC) and suicides or suicide attempts (ST) or suicidal thoughts are very rare and therefore a fortiori the quantification of forced suicides of women victims of VSC which is in fact non-existent. We will base the estimate made in this deliverable on the few existing studies.
Some previous studies:
According to various studies from Europe and the rest of the world, the physical and psychological health impact of intimate partner violence is significant. The mental health of the victims is seriously weakened, with greater risks of developing:
Anxiety (Coker et al., 2004; Pico-Alfonso et al., 2006 Hirigoyen, 2009;
Cavanaugh et al., 2011; Change et al., 2018);
Sleep disorders (Hirigoyen, 2009);
Eating disorders (Chang et al., 2018);
Psychosomatic disorders (headaches, chronic pain, difficulty breathing, etc.) (Hirigoyen, 2009);
An addiction (Chauvin, 2002; Coker et al., 2004; Pico-Alfonso et al., 2006; Cavanaugh et al., 2011; Chang et al., 2018) (more than in the case of sexual violence suffered in the childhood) (chauvinist, 2002);
Depression (Coker et al., 2004; Pico-Alfonso et al., 2006; Cavanaugh et al., 2011; Devries et al., 2013; Chang et al., 2018) (more than in cases of sexual violence suffered childhood) (Chauvin, 2002) (more than half of female victims) (Hirigoyen, 2009).
Suicide risk is also predicted by intimate partner violence according to several longitudinal studies (Devries et al., 2013). Indeed, there is a strong correlation between violence between partners and suicidal ideation (Pico-Alfonso et al., 2006; Chan et al., 2008), through depression (Chan et al., 2008). 76% of the victims of the Citoyenne féministe survey (2019) had suicidal thoughts, this would be more than 7 times the rate found among non-victims (Afifi, et al., 2009, cited by Cavanaugh et al., 2011) . According to studies (Chan et al., 2008; Cavanaugh et al., 2011; Citoyenne féministe, 2019), 20% to 29% of victims of intimate partner violence had attempted suicide at least once. The rate would be 5 to 8 times higher than the rate for the general population (Chauvin, 2002; Hirigoyen, 2009).
The risk of suicidal behavior would vary depending on:
The presence in the victim of a chronic or disabling disease, multiplying them by 2, 4, and possibly due to greater social isolation and control by the spouse (Cavanaugh et al., 2011) ;
Age, with the youngest being more at risk (Cavanaugh et al., 2011);
Ethnicity, since African Americans had a 40% lower risk than Latin Americans (Cavanaugh et al., 2011);
Suicidal behaviors of the spouse (Cavanaugh et al., 2011);
Severity (Coker, et al. 2002; Sato-DiLorenzo & Sharps, 2007, cited by Cavanaugh et al., 2011), including potential lethality (Sato-DiLorenzo & Sharps, 2007, cited by Cavanaugh et al., 2011), of the violence suffered.
However, according to Pico-Alfonso et al. (2006), the impact of violence would be identical whether it is solely psychological or both psychological and physical.
Hope could be both a protective factor and a risk factor. The latter case because too much hope could lead to more vulnerability to the accumulation of stressful life events (Chang et al., 2018).
These findings can be explained: because of the fact that in the event of fear for their life, victims may consider suicide as the only means of exercising control over a situation that has become untenable (Cavanaugh et al., 2011; Citoyenne féministe, 2019); the feeling that suicide is the only solution to end the pain felt; the desire to find “peace”; willingness to comply with the abuser’s expectations; feeling unable to live without the perpetrator; or even the multiplication of constraints (Citizen féministe, 2019).
According to Wolfort-Clevenger and Smith (2017), the coercive control present in certain situations of intimate partner violence is strongly associated with suicidal behaviors, a link explained by the theory of fluid vulnerability.
In the 2004 study by Sylvia Walby (University of Leeds – UK) “The cost of domestic violence”, it is reported that there is evidence of a strong association between domestic violence and attempted suicide. In the UK, 1,497 deaths of women by suicide were recorded in 2000, and after investigation 188 were directly attributable to VSC, or 12.5%.
The 2008 study by Prystel (France) conducted as part of a European DAPHNE project “Estimation of mortality from domestic violence in Europe” takes into account, for France, data from the ENVEFF survey providing the rate suicide attempts among women who had suffered serious violence and among those who had suffered very serious violence. The study concludes that a suicide rate of 13% is directly related to VSC.
The most recent specific study on the subject is that of the University of Kentucky (USA). This Department of Epidemiology (Sabrina Brown and Jacqueline Seals) study, published in the January 2019 Journal Injury and Violence, was designed to determine the percentage of suicides in Kentucky between 2005 and 2015 where intimate partner issues, including violence, have been identified. Kentucky state data from the National Violent Death Record System (NVDRS) was used for this purpose. The NVDRS records information from death certificates and investigation reports from medical examiners, law enforcement, toxicology and forensic reports. The researchers took over the files of all the suicides of the period, for a total of 7,008 suicides. They thus identified 1,327 (26% of documented cases) of suicides where “problems within the couple” (separation, divorce, mistrust, jealousy, discord) and/or violence within the couple were mentioned. The study indeed distinguishes between “problems within the couple” and “violence within the couple”, the latter being one of the possible categories of the former. 575 cases of problems within the couple (physical, sexual, psychological). However, the results provided in the article are not sufficiently gendered to differentiate these results according to the sex of the deceased. The overall result, useful for our estimation, is therefore the following: in 11% of the suicides studied (43% of the 26%), intimate partner violence contributed to the suicide.
Use of Virage survey results:
The recent publication of the first results concerning psychological violence from the Violence and gender relations survey: contexts and consequences of violence suffered by women and men – known as the Virage survey, sheds new light. This survey is a large-scale survey carried out in France among 27,268 women and men aged 20 to 69 with the aim of measuring the extent of violence suffered by both women and men and to objectify their prevalence. with other information on the contexts and consequences of the violence. Data collection was conducted in 2015.
During the 12 months preceding the survey, violence in the conjugal sphere is collected by 32 questions (24 relating to insults and psychological facts, 6 on physical violence and 2 on violence sexual). The specific report prepared for this working group by the Virage team (Elizabeth Brown, Magali Maruy and the Virage team – document dated October 15, 2019) indicates that “out of 1000 women in a relationship or having been in a relationship within the year , 179 report psychological violence (insults, denigration, threatening atmosphere, economic blackmail, threat to children), 13 physical violence and 3 sexual violence, knowing that these facts can be combined, physical and sexual violence always being associated with emotional abuse”.
Psychological violence is frequent, multiple and repeated for women, indicates the team: 17.9% of women interviewed in a couple or recently separated (having had a couple relationship that lasted at least 4 months during the last 12 months) declared therefore at least one act of psychological violence in the last 12 months. Among them, 30% declared at least three incidents of psychological violence and 31% at least one frequent incident (“often”, “almost every week”, “every day or almost”). The team adds that: “Reports of physical or sexual abuse are almost always accompanied by statements of emotional abuse, including jealousy and control, insults and belittlement, threatening atmosphere.”
As for dark thoughts and suicide attempts in the last 12 months, the results from Virage are as follows: answered having repeatedly had dark thoughts, thought it would be better to be dead, or thought about hurting themselves, in the past two weeks (versus 14.5% of those who did not report psychological violence ). More than one in 200 women (0.6%) who reported acts of psychological violence said they had attempted suicide in the last 12 months, i.e. four times more than women who did not report violence (0.15%) “.
The report contains many other useful data, but we note two essential findings: 17.9% of women in a relationship or recently separated report having suffered at least one act of psychological violence in the last 12 months. These facts can be multiple (in 30% of cases) and frequent (in 31% of cases). Furthermore, reports of physical and sexual violence are always associated with reports of psychological violence.
It is from these elements that we will be able to carry out our calculation. So we know that:
out of 1,000 women (aged 20 to 69) in a couple or having been one during the year, 179 report psychological violence = 17.9%;
0.6% of women who reported acts of psychological violence said they had attempted suicide in the last 12 months;
French data from the 2017 census published by the National Institute of Statistics and Economic Studies (INSEE) show the number of women aged 20 to 69 living with a partner.
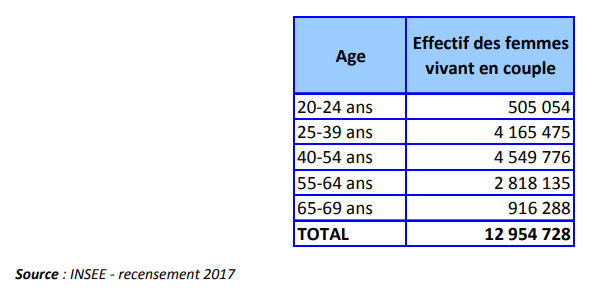
The main characteristic of violence leading to forced suicide is to be repeated psychological violence. We know that among women who are victims of psychological violence (17.9%), at least 31% do so frequently. We can therefore deduce the number of women aged 20 to 69 living in a couple and victims of repeated psychological violence: 12,954,728 * 0.179 * 0.31 = 718,858. Among them, 0.6% declared TS in the 12 last months, evening 718,858 * 0.006 = 4,313. In addition, we can know the total number of TS among women in this age group based on the hospitalization rate of women for TS by age group:
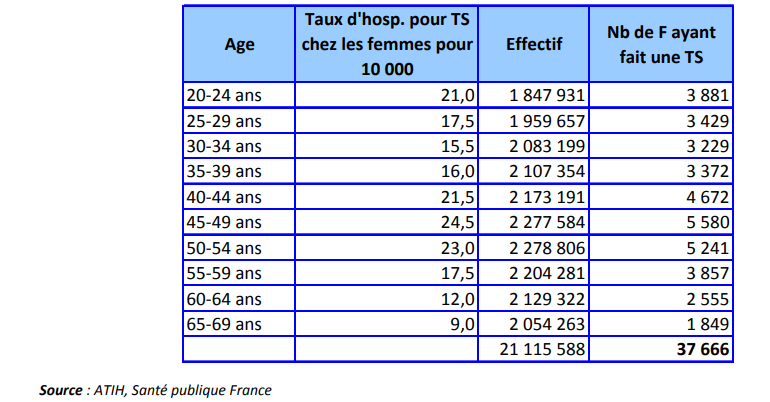
We can therefore calculate the % of TS attributable to psychological violence occurring within the couple among all TS for women aged 20 to 69: 4,313/37,666 = 11.5%;
Ultimate findings that, although there are few figures on the subject, the results of these studies converge towards a common order of magnitude between 11% and 13% of TS attributable mainly to violence within the couple. It is this lower bound of 11% that we will use for the rest of our calculations.
Method used:
We cannot, of course, have direct ex post access to the reasons that led a human being to commit suicide. Unfortunately, it is too late to have his testimony. “Psychological autopsies” which are by definition “a post‐mortem investigative procedure aimed at establishing and evaluating the risk factors for suicide present at the time of death, with the aim of determining with the highest degree of certainty the mechanism having leads to death” are still too rare to be used in a quantitative approach. On the other hand, we can know better, although still imperfectly, the reasons that led women to undergo ST, this is what we saw in the previous chapter. It is well known that the reasons for suicide are multifactorial, however, epidemiological studies learn that the strongest predictor of suicide is having ever had a ST. There is therefore a very powerful link between suicide and TS, the same causes producing the same effects in more extreme. This is how, for lack of another more scientifically assured method, we We are led to formulate the hypothesis of the same distribution of the causes of TS in the causes of suicides.
The testimonies collected in many cases of proven forced suicide, of which we have provided a few examples in the previous deliverable “Inventory of the concept of forced suicide in Europe”, confirm our assumptions that psychological violence within the couple can be the main cause of a passage to the act. The comorbidities generally associated with these acts (depression, anxiety disorders, etc.) can also be interpreted as consequences of this violence.
This “lack of anything better” reason scientifically, associated with epidemiological studies on the causes of TS and the observations made in the observations of cases conducted by experts in matters of violence within the couple, leads us to validate the hypothesis of a percentage of suicides attributable to violence within the couple at least around 11%. This figure only applies to countries in the Europe and America regions (as defined by the WHO) because of the few studies on which it is based (United States, United Kingdom, France).
Estimated number of SF in Europe:
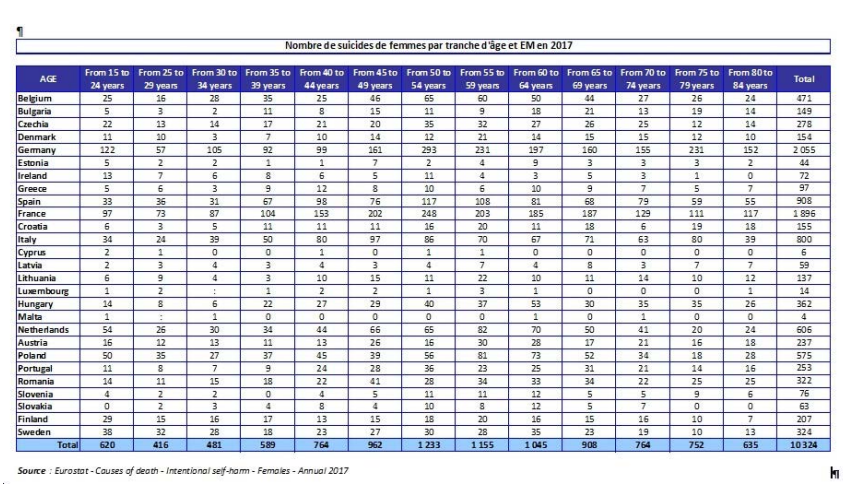
We therefore start from the examination of the number of female suicides by age group for the EU27 MS provided by Eurostat for 2017 which is the most recent year with complete mortality figures published (Causes of death – deaths by country of residence and occurrence) for these country. The raw data are as follows concerning female suicides:
Applying our 11% SF percentage uniformly to all female suicides in MS, we get the table below:
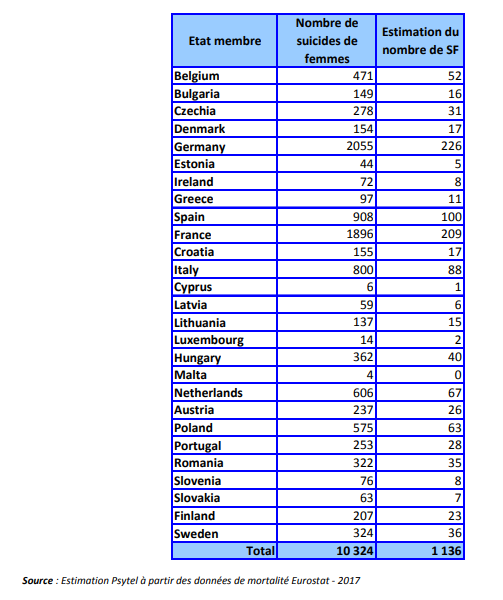
We therefore observe that:
the number of forced suicides in France in 2017 is estimated at 209;
the number of forced suicides in Belgium in 2017 is estimated at 52;
the total number of forced suicides in EU27 MS in 2017 is estimated at 1,136.
The consequences on the number of feminicides in France in 2017:
The figures produced each year since 2006 by the Delegation for Victims (DAV) of the General Directorates of the National Police and the National Gendarmerie on violent deaths within the couple are essential for determining the number of victims. Thus, for 2017, we have the following figures regarding violent deaths:
Female victims within the couple (feminicides): 130 Male victims within the couple: 21 Child victims: 25 Collateral victims: 12
These data remain incomplete due to the fact that we lacked a figure for women’s suicides, the main cause of which is the violence they suffer within the couple, “forced suicides”, as the ultimate consequences of psychological, physical and/or sexual suffered. By adding to this data our estimate of the number of SF for France in 2017, we obtain:
Female victims within the couple (feminicides): 130 Female victims of forced suicide: 209, for a total of 339 deaths of female victims of SCV for 2017.
We deliberately excluded from this total the suicides of the perpetrators of the homicides so as not to group together in the same total the victims and the perpetrators of the crimes, nor the children and collateral victims in order to limit ourselves to the sole number of female victims. However, it is true that we add together observed figures (those of the DAV) and estimated figures (those of forced suicides), but we are thus certainly closer to reality than with the only observed figures.
It is therefore nearly one female victim per day that violence within couples in France in 2017 and not one every 3 days, as is usually reported if we consider only feminicides restrictively.
The consequences on the number of feminicides in Belgium in 2017:
In Belgium, there are on average around forty feminicides per year, but there are still no official records from the public authorities. This is a press census carried out by the associations via the “Stop Féminicide” blog: http://stopfeminicide.blogspot.com/. The Stop Féminicide blog was created and is updated by the Feminist Platform against Violence Against Women. This platform brings together organizations independent of governments and political parties who wish to reflect on and act against violence against women in Belgium, through a feminist reading and approach. This blog lists the crimes, puts faces to the figures and this in order to put pressure on the public authorities. Thus, for 2017, we have the following figures concerning violent deaths: Female victims within the couple (feminicides): 43; Child victims: 4.
These data remain incomplete due to the fact that we lacked a figure for women’s suicides, the main cause of which is the violence they suffer within the couple, “forced suicides”, as the ultimate consequences of psychological, physical and/or sexual suffered. Adding to this data our estimate of the number of SF for Belgium in 2017, we obtain: Female victims within the couple (feminicides): 43; Female victims of forced suicide: 52; i.e. a total of 95 deaths of female victims of VSC for 2017.
We have deliberately excluded child victims from this total in order to limit ourselves to the number of female victims. However, it is true that we add together observed figures (those unofficial listed in the press by associations) and estimated figures (those of forced suicides), but we are thus certainly closer to reality than with the only observed figures.
It is therefore nearly one female victim every 4 days that violence within couples in Belgium in 2017 results in and not one every 10 days, as is usually reported if we consider femicides only restrictively. In Europe EU27, more than 1,000 deaths of women by forced suicide must be added to the number of victims of feminicide. We therefore call on the political authorities, the media and associations to refer to this figure which is much higher, and unfortunately closer to reality, than the already unbearable figures usually quoted.
The limits of the estimate:
By following the steps of our reasoning to arrive at our estimate of the number of SFs, we have successively:
synthesized the too few studies on the possible causes of suicide attempts in women;
determined a percentage of TS attributable mainly to VSC;
hypothesized that this percentage of cause of TS could be applied to the causes of completed suicides themselves;
- applied this same percentage to all MS in Europe EU27.
We have also applied a prudential rule by choosing the lower limit of the percentage of cause of TS attributable to VSC, being aware that the number of suicides noted in the official mechanisms for declaring the causes of mortality is systematically underestimated, by explaining clearly our calculation procedure and its possible weaknesses.
We are aware that this encryption mechanism is not scientifically assured, but that it leads to a “reasoned order of magnitude”. It seems to us that we are closer to the truth concerning the extent of the number of deaths of women victims of VSC by including this figure than by excluding it!
Ways to improve it: There are several ways to improve the robustness of our methodology:
Proposal 1: Conduct in-depth and specific studies in France and other MS on the link between VSC on the one hand and suicide attempts on the other hand to better shed light, understand, quantify and prevent forced suicides. This project contributes to this.
Proposal 2: Systematically record data concerning possible VSC in post-suicide police or gendarmerie investigations, while of course “gendering” the data collected. This amounts to systematizing psychological autopsy procedures to better investigate the causes of suicides.
Proposal 3: Raise awareness and train front-line personnel (police, gendarmes, firefighters, emergency personnel) on the existence and detection of suicide attempts in connection with violence within the couple.
Studies on the link between violence within the couple and suicide or TS:
It is essential to consider intimate partner violence as a public health problem. Indeed, according to WHO figures, women victims of intimate partner violence lose one to four years of healthy life. In addition, this violence multiplies by two health care expenses for these women. It is also important to specify that the costs of domestic violence would amount to the impressive figure of 16 billion euros in Europe.
Several studies have set themselves the objective of analyzing the consequences of violence between intimate partners on the mental health of women, some of which have highlighted the correlations between this violence and suicide attempts made by female victims. A presentation of these articles is given in the following lines. Note: We logically assume that the figures given in the articles relate to the life until then when no other duration is mentioned.
- Articel n°1 : Morvant, C., Lebas, J., & Chauvin, P. (2002). Les conséquences des violences conjugales sur la santé des femmes et leur prise en charge en médecine de premier recours. Retrieved from https://www.researchgate.net/profile/PierreChauvin/publication/10900409_Consequence
s_of_domestic_violence_on_women%27s_health_and_their_management_in_primary_health_care/links/5c8fc216299bf14e7e844d97/Consequences‐of‐domestic‐violence‐on‐womens‐health‐and‐their‐management‐in‐primary‐health‐care.pdf [France]
A 2002 study analyzing the consequences of domestic violence on women’s health came to some conclusions. First of all, it is important to note that half of women who are hospitalized in psychiatry suffer from violence from their partner. In addition, the risk of post-traumatic syndrome and depression appears to be greater in contexts of domestic violence than sexual violence suffered in childhood. The same is true for the consumption of psychotropic drugs, which is very high among these female victims. It is, in fact, 4 to 5 times higher compared to the general population. Finally and more fundamentally, as a consequence of the previous elements, they would make 5 times more suicide attempts compared to the general population.
- Articel n°2 : Cavanaugh, C. E., Messing, J. T., Del‐Colle, M., O’Sullivan, C., & Campbell, J.C. (2011). Prevalence and Correlates of Suicidal Behavior among Adult Female Victims of Intimate Partner Violence. Retrieved from https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3152586/pdf/nihms282593.pdf [USA]
This study aimed to highlight the prevalence and correlates of suicide threats and suicide attempts among 662 women victims of intimate partner violence. According to the National Institute of Health, women who experience intimate partner violence have more likely to have suicidal thoughts and/or behavior. Indeed, a study reveals that female victims are 7 times more likely to present suicidal thoughts compared to women who are not confronted with this type of violence. Furthermore, one in five victims threatened or attempted suicide in their lifetime. The article adopts an interesting intersectional perspective.
Thus, women suffering from a chronic or disabling illness were 2.4 times more likely to have threatened or attempted suicide than others. These data can be explained by the fact that these people may be more socially isolated and controlled by their spouse and may therefore see suicide as the only way out. Younger women are significantly more affected.
Ethnicity is also an important variable since African American victims are 40% less likely to have threatened or attempted suicide than Latin Americans. In addition, certain circumstances can increase the risk of victims of violence threatening or attempting suicide.
For starters, victims at higher risk of experiencing life-threatening assaults from their intimate partners are significantly more likely to have threatened or attempted suicide.
In addition, serious abuse inflicted by the spouse as well as the dangerousness of the spouse also have an impact.
These findings can be explained by the fact that in the event of fear for their life, victims may consider suicide as the only means of exercising control over a situation that has become untenable. The considerable danger incurred in the context of an abusive relationship impacts the mental health of women who are victims who are more likely to suffer from post-traumatic stress disorder, anxiety and depression. These consequences attached to serious violence on the mental health of women aggravate, in turn, the likelihood that victims will have suicidal thoughts.
Finally, it appeared that female victims whose spouse had threatened or attempted suicide had a higher risk of having threatened or attempted suicide themselves.
- Articel n°3 : Devries, K.. M., Mak, J. Y., Bacchus, L. J., Child, J. C., Falder, G., Petzold, M., Astbury, J., & Watts, C. H. (2013). Intimate Partner Violence and Incident Depressive Symptoms and Suicide Attempts: A Systematic Review of Longitudinal Studies. Retrieved from https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3646718/pdf/pmed.1001439.pdf [USA, Australie, Inde, Suède, Nicaragua, Afrique du Sud].
This systematic review and meta‐analysis, including longitudinal studies published before February 2013, aims to investigate the links between intimate partner violence and depression and suicide attempts, and vice versa.
Some studies have, on the one hand, found that contexts of intimate partner violence were strongly and consistently associated with depressive disorders and suicides. A survey found that intimate partner violence doubled the risk of suffering from depressive symptoms.
On the other hand, there are associations in the opposite direction. An analysis showed that depressive symptoms doubled the risk of women experiencing domestic violence.
The present study confirms this bidirectional direction: women with depression are more likely to be in an abusive relationship, but being in an abusive relationship predicts a depressive disorder and thus increases the risk of a suicide attempt.
- Articel n°4 : Citoyenne Féministe. (2019). Violences conjugales : dépression et envie suicidaire. Retrieved from https://static.mediapart.fr/files/2019/10/02/enquete‐cf‐violences‐ conjugales‐et‐envie‐suicidaire.pdf [France].
The “Citizen Feminist” movement aimed, in this investigation, to highlight the phenomenon of forced suicides. 584 victims responded to an online questionnaire.
It appears from his study that 76% of the victims declared having had suicidal thoughts, that 29% of them made suicide attempts and that 13% were hospitalized in psychiatry.
These figures can be explained by several reasons: the feeling that suicide is the only solution to end the pain felt; the will to find “peace”; the urge to regain control through suicide; willingness to comply with the abuser’s expectations; the feeling of being unable to live without the perpetrator or the multiplication of constraints.
- Articel n°5 : Hirigoyen, M.‐F. (2009). De la peur à la soumission. Retrieved from https://www.cairn.info/revue‐empan‐2009‐1‐page‐24.htm [France]
This article aims to highlight the devastating effects of domestic violence on the health of women who experience it.
Violence between intimate partners can, first of all, cause psychological disorders such as anxiety, sleep disorders, difficulty concentrating, etc. These difficulties lead, for many of these women, to heavy consumption of alcohol, toxic or even psychotropic drugs.
A number of psychosomatic disorders can also present themselves. Some female victims may suffer from chronic pain, headaches, breathing difficulties, etc.
It is important to highlight that depression affects more than half of women victims of violence from their spouse. They would also make 5 to 8 times more suicide attempts compared to the general population.
- Articel n°6 : Chan, K. L., Straus, M. A., Brownridge, D. A., Tiwari, A., & Leung, W. C. (2008). Prevalence of dating partner violence and suicidal ideation among male and female university students worldwide. Retrieved from http://hub.hku.hk/bitstream/10722/60541/1/Content.pdf [21 pays]
This is a survey aimed at measuring the proportion, within a large sample of students, of people who have perpetrated physical and/or sexual violence against their intimate partner. It was also a question of making the link between domestic violence and suicidal thoughts.
The study shows that there is a strong correlation between intimate partner violence and suicidal ideation, both on the side of perpetrators and victims. It is depression that explains the relationship between dating violence and suicidal ideation.
The survey also highlighted the fact that women exposed to intimate partner violence are more likely than others to have attempted suicide. Rates of suicide attempts among female victims range from 20 to 26%.
- Articel n°7 : Chang, E. C., Yu, E. A., Kahle, E. R., Du, Y., Chang, O. D., Jilani, Z., Yu, T., & Hirsch, J. K. (2018). The Relationship Between Domestic Partner Violence and Suicidal Behaviors in an Adult Community Sample: Examining Hope Agency and Pathways as Protective Factors. Retrieved from
https://www.researchgate.net/publication/320289498_The_Relationship_Between_Domestic_Partner_Violence_and_Suicidal_Behaviors_in_an_Adult_Community_Sample_Examining_Hope_Agency_and_Pathways_as_Protective_Factors/link/5c34bca8299bf12be3b798d3/download [USA]
98 people aged 18 to 64 took part in this study aimed at determining the links between hope, domestic violence and suicidal ideation. Domestic violence has a heavy impact on the mental health of women who experience it. They are, in fact, more likely to suffer from, among other things, depression, anxiety, eating disorders and post-traumatic stress. Studies have shown that 20% of female victims of intimate partner violence had threatened or attempted suicide in their lifetime. Although it is known that intimate partner violence can worsen suicidal behavior, few studies were conducted to determine potential protective factors that might reduce the risk of them engaging in these behaviors. This is why this article aims to determine to what extent hope could have an influence both on domestic violence and on the risk that it leads to suicidal behavior. The results of the study that was conducted go in two opposite directions: hope can indeed attenuate the relationship between domestic violence and suicidal behavior but it can also exacerbate it. An explanation for understanding the second effect is as follows: the fact, for a person, having a high level of hope can make them more vulnerable when faced with an accumulation of stressful life events, such as during experiences of domestic violence. However, further studies are needed to understand to what extent hope may be more or less beneficial for victims of intimate partner violence.
- Articel n°8 : Wolford‐Clevenger, C., & Smith, P. N. (2017). The Conditional Indirect Effects of Suicide Attempt History and Psychiatric Symptoms on the Association Between Intimate Partner Violence and Suicide Ideation. Retrieved from http://europepmc.org/backend/ptpmcrender.fcgi?accid=PMC5647881&blobtype=pdf [USA]
The purpose of this survey was to deepen the understanding of the link between violence between intimate partners and suicidal behavior, more specifically in the situation of women seeking shelter with ad hoc professionals. The study aimed to interrogate the impact of coercive control on suicidal thoughts. 134 women participated in this cross-sectional study. The survey highlights that victims seeking shelter are at an increased risk of having had suicidal thoughts and attempted suicide (34%) compared to both other victims who do not seek such help (6 .6%) than to women in the general population (4.2%). These results may, among other things, be justified by the fact that these women are subject to coercive control by their spouses.
The concept of coercive control refers to: “repetitive strategies, some violent and some not, the cumulative effects of which must be analyzed in their larger context of domination”.
It unfolds through two mechanisms.
On the one hand, the perpetrator may resort to coercion. The latter refers to any strategy adopted by the perpetrator of violence in order to get what he wants in the immediate future. The use of force or the threat to use it are methods that can be employed in this regard.
On the other hand, the aggressor can use the control strategy. Control takes the form of a series of strategies that can take place at different times during the relationship. They can materialize through deprivation of rights and resources and the imposition of micro-regulations. The latter refer to rules dictated by the executioner which can take multiple forms and which aim to maintain the control and domination of the perpetrator over his victim.
Thus, unlike violence between intimate partners, which manifests itself in acts that take place according to a certain gradation and in an episodical manner, the notion of coercive control refers to the cumulative and invisible strategies that the spouse puts in place, some of which may be seen as less serious.
Numerous studies have, in fact, shown that coercive control is strongly associated with suicidal ideation and behavior.
It is the theory of fluid vulnerability that would help to understand the links between coercive control, psychiatric symptoms and suicidal behaviors. According to this theory, “stressors activate acute vulnerability to suicide through a ‘mode suicidal”, which involves distinct, suicide-promoting responses from the cognitive, affective, physiological, and behavioral/motivational systems”. “Specifically, cognitive responses involve one or more negative core beliefs, such as worthlessness and hopelessness. The affective system is characterized by dysphoria, involving various negative mood states such as sadness, anger, and anxiety. The physiological components of this mode involve heightened arousal. The behavioral and motivational aspects of the suicidal mode involve a clear desire for death or the intention to end one’s life. It is important to note that previous suicide attempts will create a lasting vulnerability thus predisposing the female victims to the activation of the suicidal mode. The latter will thus be activated more often by victims who have made several suicide attempts than by those who have made only one or have not made one due to the existence of this vulnerability to the suicidal mode. Women in controlling relationships may be vulnerable to negative self-directed thoughts. It thus appears that victims who seek help suffer from depressive symptoms, post-traumatic stress disorder, despair, etc. According to the theory of fluid vulnerability, these disorders increase the risk of adopting suicidal behaviors.
- Articel n°9 : Coker, A. L., Smith, P. H., Thompson, M. P., McKeown, R. E., & Bethea, L. (2004). Social Support Protects against the Negative Effects of Partner Violence on Mental Health. Retrieved from https://uknowledge.uky.edu/cgi/viewcontent.cgi?referer=&httpsredir=1&article=1114&co
ntext=crvaw_facpub [USA]
This survey was conducted among 1,152 women victims of intimate partner violence, whose ages ranged from 18 to 65 years in family medicine clinics between 1997 and 1999. The objective pursued was to determine what was the impact of violence on health mental health of victims and to what extent social support could reduce this impact.
Intimate partner violence has consequences for the mental and physical health of victims. The latter are, in fact, more likely to suffer from drug dependence, symptoms of post-traumatic stress, depression, anxiety and behaviors. suicidal.
It appears from this survey that, among women who testified to the violence suffered from other people, those who received support from these people presented a reduced risk of having thoughts or adopt suicidal gestures. These victims were less likely to have poor mental or physical health.
- Articel n°10 : Pico‐Alfonso, M. A., Garcia‐Linares, M. I., Celda‐Navarro, N., Blasco‐Ros, C., Echeburua, E., & Martinez, M. (2006). The Impact of Physical, Psychological, and Sexual Intimate Male Partner Violence on Women’s Mental Health: Depressive Symptoms, Posttraumatic Stress Disorder, State Anxiety, and Suicide. Retrieved from https://www.liebertpub.com/doi/pdf/10.1089/jwh.2006.15.599 [Espagne]
This study aimed to establish the impact of intimate partner violence (physical, psychological and sexual) on the mental health of victims. To do this, a comparison between 75 physically and psychologically abused women; 55 women psychologically abused; and 52 non‐abused women; was conducted.
It appears that women victims of violence (whether physical and psychological or only psychological) have a higher risk of presenting depressive and anxious symptoms, post-traumatic stress and suicidal thoughts.
It should be noted that, according to this study, there is no difference in terms of impact on the health of victims between those exposed to physical and psychological violence and those exposed only to psychological violence. These results seem important in the insofar as moral violence is still strongly considered to be violence of lesser gravity within the collective unconscious.
- Articel n°11 : Mason, R., & O’Rinn, S. E. (2014). Co‐occurring intimate partner violence, mental health, and substance use problems: a scoping review. Retrieved from https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4240863/pdf/GHA‐7‐24815.pdf [Canada]
This literature review identified 35 articles examining the link between intimate partner violence and mental health, published between 2004 and 2014. The objective of this work was to inform frontline mental health professionals what is had to know to provide appropriate care for women victims of intimate partner violence.
Declared epidemic in 2002 by the WHO69, violence between partners, which mainly affects women, also takes on different forms and has more severe consequences for women.
In particular, emotional or psychological abuse has been associated with low self-esteem, depression and post-traumatic stress disorder. The risk of femicide has been associated with the presence of both depression and post-traumatic stress disorder. Alcohol use by the victim, on the other hand, was not associated with lethal risk. Indeed, in another study, victims who suffered the most severe forms of violence were more likely to have comorbidities. One possible explanation for the links between childhood and adult abuse and substance use is that childhood abuse can lead to low self-esteem, depression, anxiety, guilt and other issues. psychological, which in turn result in vulnerability to adult victimization and self-medication via the products.
There are around 2,000 suicides per year in Belgium. Suicide is the 7th cause of death for the total Belgian population, all these causes combined. When referring to “external” causes of death, this phenomenon represents the leading cause of death. It is important to specify that most of the statistics relate only to completed suicides. There is, in fact, no official record of attempted suicides, which are estimated to be 10 to 20 times more numerous. It is, however, necessary to be cautious with these figures due to the existence of an underestimation in the number of deaths caused by suicides.
The reasons are the absence of precise criteria for declaring suicides and the lack of autopsies which would have allowed an identification of the cause of death. The propensity to declare a suicide can vary depending, in particular, on the doctor in charge of the certification, on cultural or religious criteria of the deceased person or his entourage. The same is true for reports of attempted suicides which are much lower than the reality.
Certain groups more affected?
Gender criterion
The gender criterion has a strong impact in the phenomena of suicides and attempted suicides. Completed suicides concern, for the most part, men. Men commit suicide, about three times more than women.
Regarding suicide attempts, the trend is reversed: it is women who are much more affected. Indeed, the proportion of suicide attempts rises from 1 to 3 for men and from 1 to 14 for women.
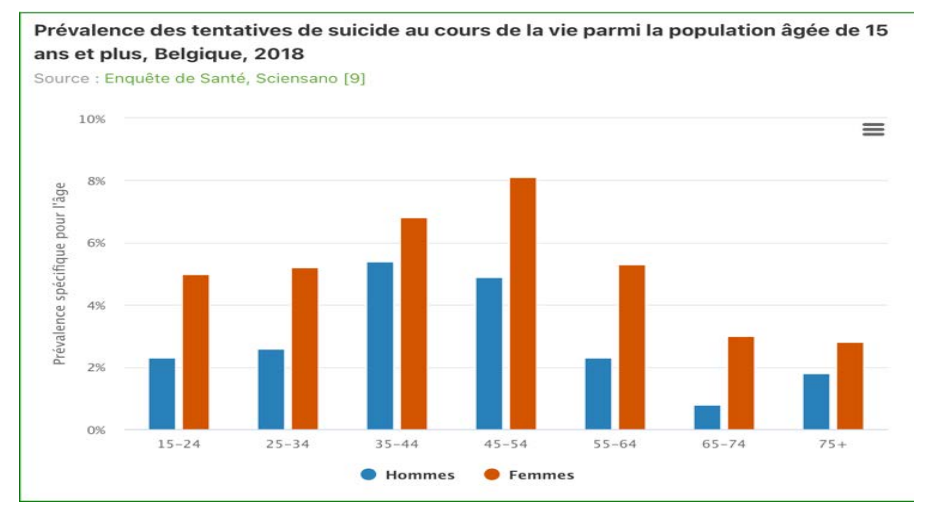
Meanwhile, according to a 2017 survey, more women reported having had suicidal thoughts in their lifetime compared to men (16% vs. 12%).
Women therefore contemplate and attempt to end their lives more, while more men succeed in doing so. The figures support this reality: 1243 suicides were recorded among men against 500 among women.
The reasons for these higher suicide rates among men appear to be primarily societal. Men have more impulsive behavior than women. They would also have more recourse to violent means to end their lives such as firearms, hanging or even explosives, while women would prefer more drug ingestion. In addition, women would be safer from emotional and social isolation due to the fact that they are still more involved in the family sphere. Finally, it appears that men have more difficulty asking for help when they need it and also use medical and support services less.
Age criterion
The people most affected by suicidal behavior are adolescents and the elderly. There are, in fact, a significant number of suicide attempts in adolescence and completed suicides among the elderly. Thus, among young people under 25, there are 100 to 200 suicide attempts. Concerning people aged over 65, suicides concern 1 in 2 or 3 people.
Qualification level criterion
Suicidal behavior is also linked to the level of education of the people concerned. People with the least education are 1.5 times more likely to think about suicide during their lifetime than people with the highest level of education. According to a survey carried out in 2008, there are more suicide attempts among the least educated. There are thus 6.7% in the group of people who have received the least training compared to 4.1% of higher education graduates. Evolution of the workforce: The mortality rate linked to suicide is stable among men and tends to decrease among women, at least in Wallonia. There is thus a rate equivalent to 0.33 among men and a rate which fell from 0.14 in 1989 to 0.10 in 2004 among women.
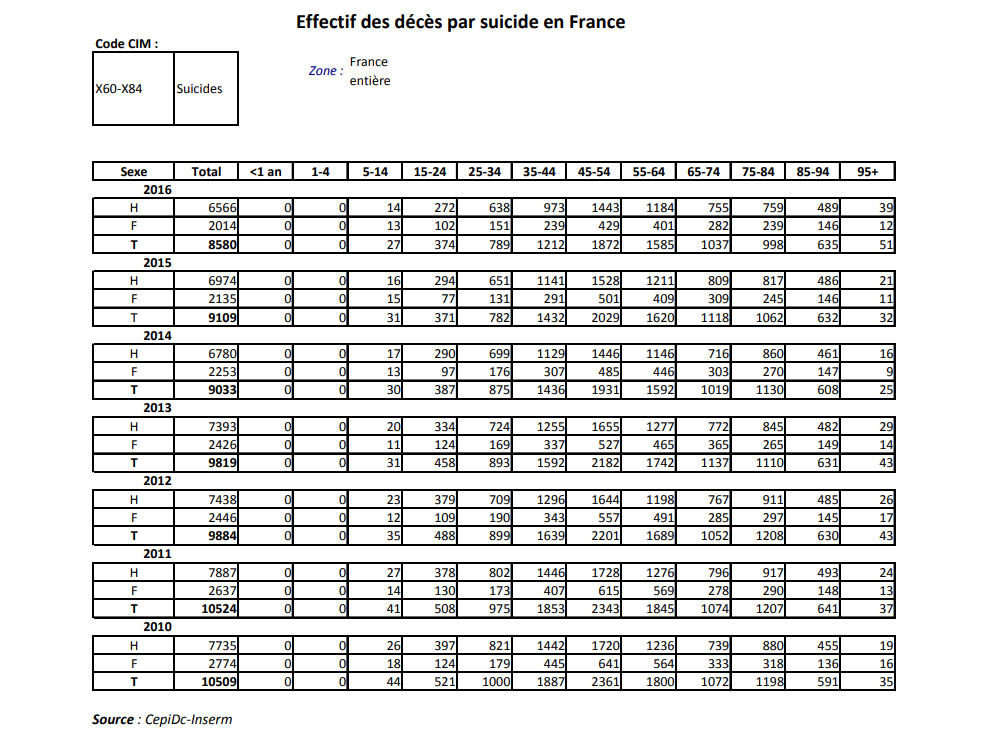
With approximately 8,500 deaths by suicide per year, France has a higher suicide rate than the European average. It is therefore a major public health problem with a significant impact in human and economic terms. To this figure must be added approximately 100,000 suicide attempts giving rise to contact with the healthcare system per year. France is therefore one of the European countries most affected by this scourge. Figures on suicides are provided in France by the CépiDc of Inserm (Epidemiology Center on medical causes of death). Mortality data come from the declaration and coding of the causes of death. They have been collected officially and regularly in France since 1968. We present below the tables of the numbers of deaths by suicide of the CépiDc from 2010 to 2016, according to age and sex:
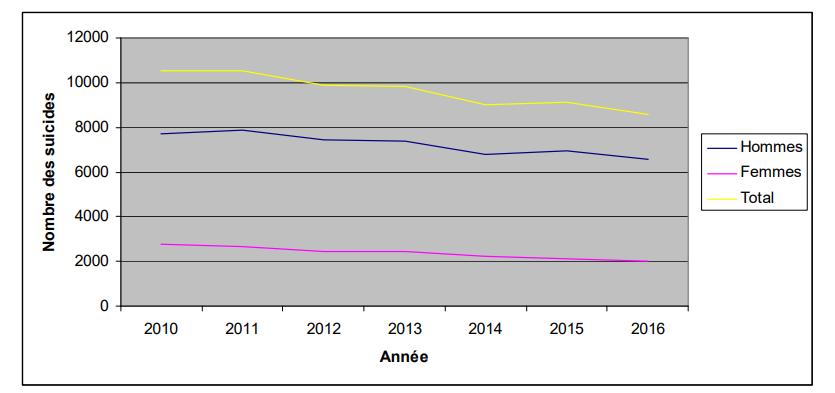
Here is the graph of the evolution of these numbers during this period:
Suicide attempts (TS) in France:
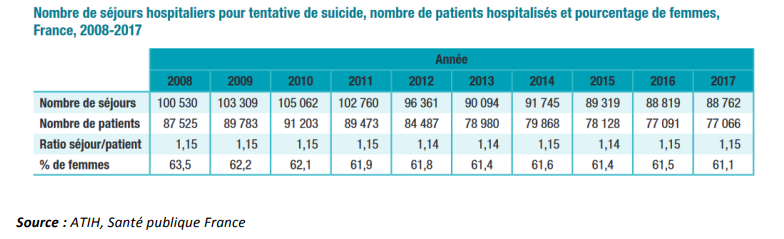
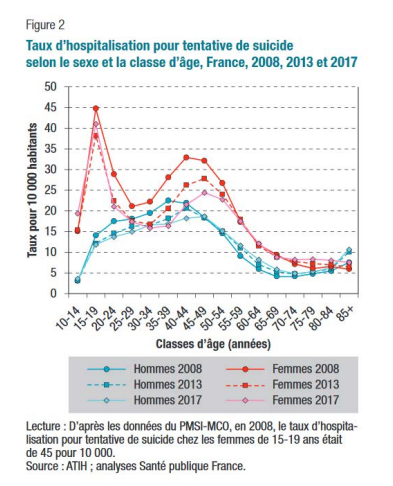
A 2019 thematic publication of the Weekly Epidemiological Bulletin (BEH) published by Public Health France reports that: “nearly 5% of 18-75 year olds in the general population report having thought about committing suicide in the last 12 months and more than 7 % say they have had TS in their lifetime. Women were more affected than men. Several factors associated with suicidal behavior are identified: having had a depressive episode, having to deal with difficult financial situations, being single, divorced or widowed, professional inactivity, exposure to violence, as well as traumatic events in childhood. The use of data from the PMSI-MCO (Programme for the medicalization of information systems in medicine, surgery and obstetrics) makes it possible to monitor the numbers and rates of hospitalization for TS. The analysis of these data is limited to hospitalized suicide attempts in medicine and surgery departments, including stays in short-term hospitalization units (UHCD) in emergency departments. However, it does not take into account patients who went to the emergency room after a suicide attempt but were not hospitalized, nor those who are hospitalized in psychiatry, directly or after their visit to the emergency room, without prior hospitalization in a medical service. Indeed, hospitalizations in a psychiatric establishment after a suicide attempt are poorly recorded in the hospital information system. The number of hospital stays for TS in short-term facilities was more than 100,000 per year between 2008 and 2011. From that date, this number gradually decreased, reaching just under 89,000 hospitalizations in 2016 and 2017 . The relative share of women hospitalized for TS fell from 63.5% in 2008 to 61.1% in 2017, thus slightly reducing the gap between the two sexes. But the number of TS remains much higher among women than among men, unlike the number of suicides.
If we now examine the hospitalization rate for TS by age and sex (diagram below), we see that regardless of the year studied, the hospitalization rates for TS by age are higher in women than men, except over 85 years of age. This analysis confirms the worrying situation for young girls aged 15 to 19. It is in this population that the highest rate is systematically observed regardless of the year.
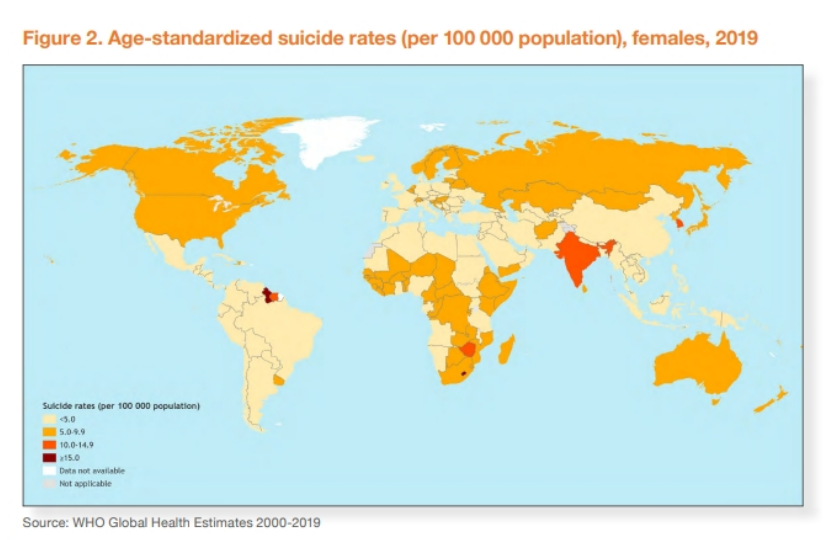
More than 700,000 suicides were recorded worldwide in 2019, according to the latest figures from the World Health Organization (WHO), i.e. one death every forty seconds. Suicide is a global phenomenon, but indeed 77% of suicides occurred in low- and middle-income countries in 2019. Suicide accounted for 1.3% of all deaths globally, making it the 17th leading cause death in 2019. It was the fourth cause of death among 15-29 year olds worldwide in 2019. It should also be noted that the number of TS is generally 20 times higher than the number of suicides. The reasons cited for these deaths vary, depending on the country, from free access to firearms in the United States to excessive alcohol in Russia. But, it should not be forgotten, reminds the WHO, that the suicide rate is much higher in low-income countries. We must also mention the specific situation of women who in many countries are locked into a heavy patriarchal system that can prove fatal for them. Thus, suicide affects men almost three times more than women in France, this is far from being the case in countries such as Bangladesh, Lesotho (in South Africa) or Myanmar (the former Burma ), where women commit suicide more than men. Finally, the country with the highest number of female suicides is India with 72,935 female deaths in 2019, a rate of 11.1 per 100,000 women. The few countries with a higher age-standardized rate of suicide mortality for women are Lesotho (34.6), Guyana (17.0) and Suriname (11.8). Below we provide the world map published by the WHO based on the age-standardized rate of female suicide mortality in 2019:
An article from The Lancet public health published in 2020, established that 37% of women who commit suicide in the world live in India. Excessive punishments, forced marriages, systemic assaults, rapes, honor killings and all types of violence against women do not fail to account for the oppression that Indian women suffer. Closer to home, in Morocco, the inequalities between women and men are glaring when examined from the angle of suicide. Out of 1,013 cases of suicide recorded in 2016, 613 concerned women. A very high percentage, but not so surprising, when certain news items testify to the way in which women’s rights are little respected in Morocco: high frequency of domestic violence, sexual harassment in the streets and on the beaches or the ban on abortion that induces forms of self-inflicted repression. The WHO Global Suicide Report (2019) states that: “While the link between suicide and mental disorders (particularly depression and alcohol use disorders) is well established in high-income countries, many suicides occur impulsively in times of crisis with a loss of ability to cope with life stresses, such as problems, relationship breakdown, or chronic pain and illness. Additionally, experiencing conflict, disaster, violence, abuse or loss and feeling isolated are strongly associated with suicidal behavior. Suicide rates are also high among vulnerable groups facing discrimination, such as refugees and migrants, indigenous populations, gay, lesbian, bisexual, transgender, intersex (LGBTI) people, and prisoners.” What should be remembered from these figures is that the phenomena of suicide and TS are major global societal facts, but with different characteristics. Thus, the percentage of TS attributable, as the main cause, to violence within the couple will be different between the major cultural and geographical regions. The rate that we are going to determine in the tab “suicides in Europe” is undoubtedly a low rate compared to, for example, the region of South-East Asia (as defined by the WHO) according to the mortality data in our possession and the cultural contexts that we perceive as even more unfavorable to women’s rights.
Remarks:
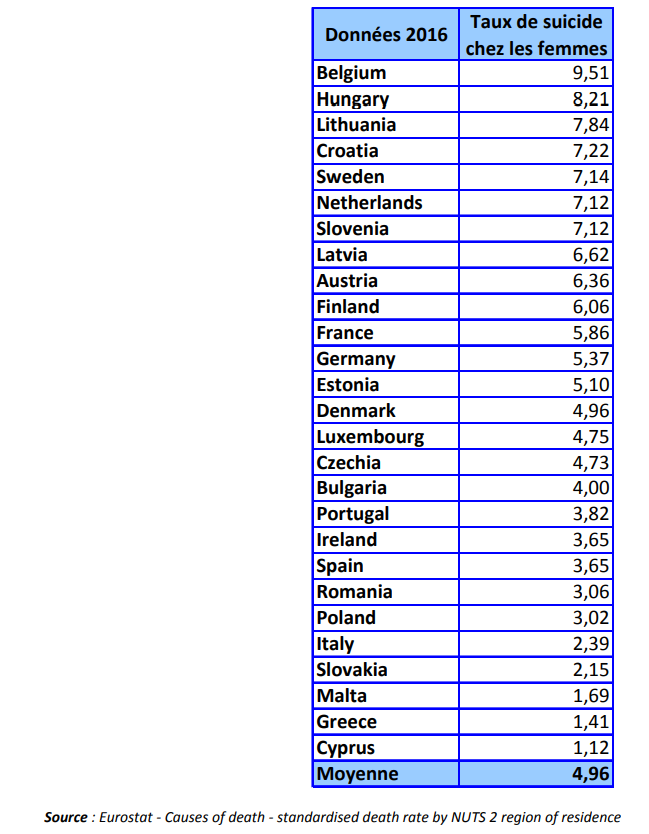
Belgium is the MS most affected by the phenomenon of female suicides with a standardized rate of 9.51 per 100,000. France with a rate of 5.86 is slightly above the average (4.96 ). The variability of this rate is significant between the different MS, since Belgium has a rate more than 8 times higher than the rate in Cyprus.


